Photo / jose leiva courtesy cmh
John Alexander, chief medical officer at Central Maine Healthcare, led the incident command response that put together the health care system’s pandemic plan.
Please do not leave this page until complete. This can take a few moments.
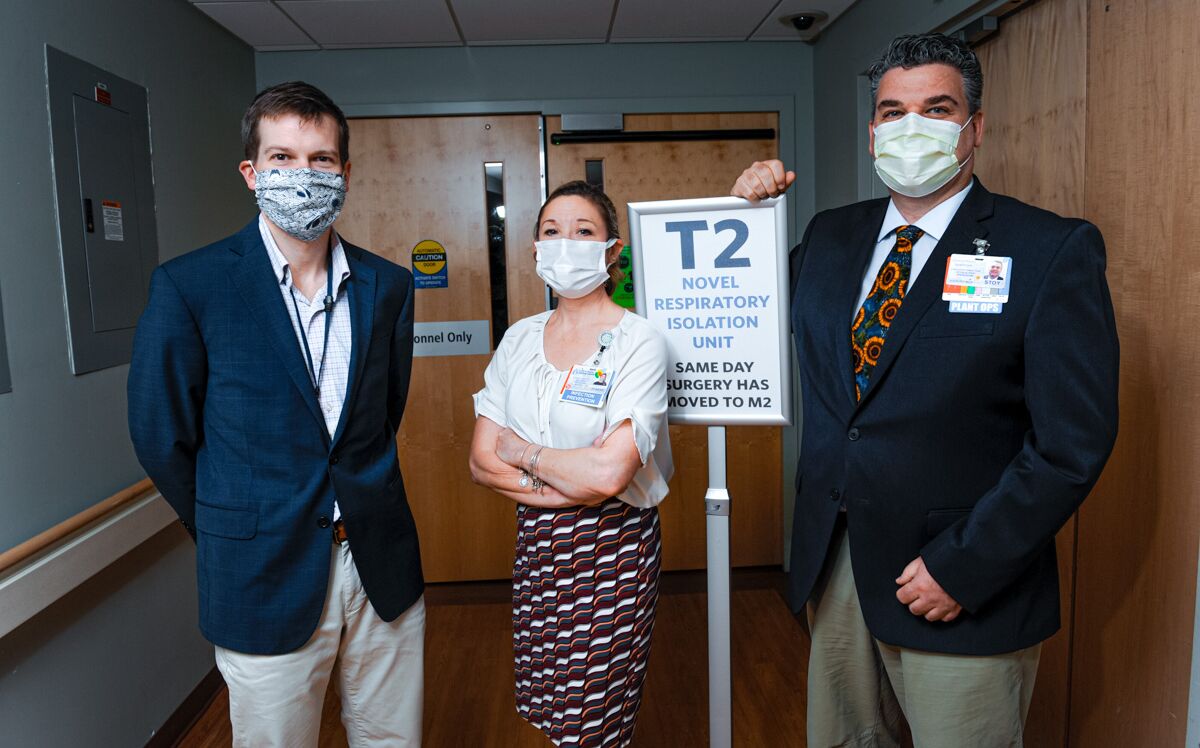 Photo / Jose leiva Courtesy of CMH
Members of CMH’s team that prepared the hospital for the COVID-19 pandemic include, from left, Sheldon Stevenson; director of emergency medicine; Joanne Kenny-Lynch, director of infection prevention; and Stoy Hancock, director of facilities management.
Photo / Jose leiva Courtesy of CMH
Members of CMH’s team that prepared the hospital for the COVID-19 pandemic include, from left, Sheldon Stevenson; director of emergency medicine; Joanne Kenny-Lynch, director of infection prevention; and Stoy Hancock, director of facilities management.
Joanne Kenny-Lynch has watched viruses for a living for nearly three decades, so she wasn’t worried in January when she started watching one in China.
But still, as director of infection prevention for Central Maine Healthcare, she brought it up at the annual leaders meeting Jan. 22. It was the day after the first reported U.S. case of the virus, which didn’t yet have a name. She and her team guide the hospital in dealing with infections, most of which never make the news.
“I was just trying to get them used to hearing about it.”
No one was thinking pandemic. “They said, ‘Oh there’s Joanne, she’s happy because she’s got another bug to play with,’” she says.
But things happened fast.
“It went from ‘Hey, look what’s going on here’ to ‘Oh boy, here it comes.’”
January was a buoyant time for CMH. After years of financial and staff upheaval, things had turned around under the leadership of CEO Jeff Brickman, who was recognized in March as a Mainebiz Business Leader of the Year.
On Jan. 25, CMH held a public meeting to introduce plans for an oncology center. A Lewiston urgent care center was set to open in March, and more expansion was on the horizon.
Behind the scenes, Kenny-Lynch was tracking the virus, sending out weekly information to departments, including a graph showing the spread.
“Each week you’d see more countries where the little blue dots were moving to, from Wuhan, China, to South Korea, to Japan, to Italy.”
She soon realized, “Wow, this is going to shake our world.”
John Alexander, CMH chief medical officer, was following the virus, too. The hospital keeps an eye on infectious diseases, like the flu, or a measles outbreak it had prepared for a few months before.
In early February, as what was now COVID-19 spread on the West Coast, he started getting questions from both inside and outside the hospital.
“That’s often one of the first things that happens,” Alexander says. “People have questions.”
By the end of February, it had snowballed, Kenny-Lynch says. “We realized this was way bigger than two departments.”
They began to check things like capacity to isolate patients at Central Maine Medical Center, in Lewiston, and the system’s hospitals in Bridgton and Rumford. They checked personal protective equipment inventory and CMH ordered HEPA negative-air systems, used to scrub the air in infected patient rooms.
At one point, Kenny-Lynch told Alexander, “I can’t do this alone anymore.”
When Alexander moved to set up a hospital incident command system, she was relieved. Structured by the Federal Emergency Management Agency, the system outlines command and communication strategy.
“It’s like, all right, it’s not just the infection prevention show, every hand on deck,” she says.
Sheldon Stevenson, an ER doctor, was preparing to begin a new role as system chief for emergency medicine.
In February, a colleague texted him about COVID-19, concerned about hospital response.
Stevenson responded that he was following it too, but there were bigger things to think about. “It’s a long way off,” he said.
On March 2, the day before he started his new job, he was watching the news when it clicked. He remembers thinking, “This is going to be a huge problem.”
The next day he attended the first informal meeting of the group that would later form incident command.
“It really evolved quickly,” he says. That day, as the new emergency medicine chief, he focused on getting his group ready for possible COVID-19 emissions. A week later, he was named head of the medical branch of the incident command team.
Stoy Hancock, was also in a new role, as executive director of facilities management, and was new to the hospital.
He’s been in health care facilities management for two decades and had pandemic training, particularly for the Ebola and SARS outbreaks. “Nothing to compare to this, though” he says.
Just days after starting his job, at the first incident command meeting on March 9, Hancock was assigned to figure out what space in the hospital could be retrofitted into a COVID-19 unit. It would need individual negative air pressure rooms, and whatever department was displaced would need a new home.
His deadline was ASAP.
“What a great way to introduce myself to the senior leadership,” he says. He was still learning the hospital layout.
Within five days the same-day surgery department had become a 14-room COVID-19 unit.
In a process he figures was 40% guidelines and 60% “MacGyver,” Hancock designed four-walled rooms out of three-sided examination bays, using heavy plastic. They had a “storm door” for safe entry and a larger zipper opening to accommodate gurneys.
The windows had to be removed, replaced with plywood, because the negative air machines need an exhaust outlet. Eventually, as the hospital created three more COVID-19 units, 55 windows were removed, including on the fourth and fifth floors, requiring an 80-foot lift.
Mary Anne Ponti, chief of nursing operations and incident command operations manager, had to put into operation what Hancock designed. She says listening to him discuss what they were going to do and how they were going to do it was “amazing.”
A nurse for 40 years, she’d never seen anything like it. “It proved to me that this team can do anything we need to do,” she says.
In Bridgton, Peter Wright, president of Bridgton and Rumford hospitals, was also following the virus. He’s chairman of the American Hospital Association policy board, which in the first week in March had a serious conversation about potential impact.
He was ready when planning started at CMH. Preparation at the hospitals, which each have 25 beds, was on a smaller scale and came with unique challenges.
“I had to plan for my hospitals, how we were going to serve our community,” Wright says. “That’s our primary responsibility.”
While there’s “tremendous depth in the ranks” at CMH, the smaller hospitals don’t have the full-time specialists, or resources, that CMMC has.
He told the staff, “Let’s remind ourselves what it is that we can handle and how much of it we can handle at once. It was a good exercise for us.”
Once planning began, “We just went to work and did what we always do, just shifted our focus from one aspect of community health to another.”
Across departments, people fell into their roles.
“People were able to take their skills, what they do with their normal day jobs, and apply it toward what we needed to do to get things done,” says Kenny-Lynch, the director of infection detection. “To change protocols and processes, basically to shut the hospital down and gear it up to one particular disease, was incredible.”
A surge plan was drawn up that could expand the system from 300 beds across the three hospitals to 450, and from 20 ICU beds to 80, says Alexander, the chief medical officer.
The plan also could triple the capacity of the morgue. “Other hospitals in metropolitan areas were dealing with it, so we had to have that plan in place,” he says.
Alexander coordinated with the chief medical officers of MaineGeneral in Augusta and St. Mary’s in Lewiston so the hospitals could help bear the others’ loads, if necessary.
“It felt like we were making plans and waiting, making plans and waiting,” he says.
That didn’t last long.
Maine’s first COVID-19 case walked through CMMC’s emergency room door on March 10.
“It came at us pretty quickly,” says Stevenson, the director of emergency medicine. The medical staff braced for a surge. “We really thought we were going to be overrun, that was our mindset.”
Alexander was relieved, in a way. “We were starting to create some level of restrictions and that’s hard to do in a public health crisis before the threat is obvious.”
At least people would know it’s real, he remembers thinking.
The case was made public by Gov. Janet Mills in a March 12 news conference, and the state began to shut down.
By the end of the week, the hospital had two more cases. Soon, the hospital would cancel elective procedures, and eventually furlough 300 employees.
On March 13, Ponti, chief of nursing operations, and her husband went out to dinner. The restaurant owner said he didn’t think the threat was real, everyone was overreacting.
“But we knew it was real,” Ponti says. “Very real.”
By early April the hospital was performing 25 to 50 tests a day, with between five and 10 a week positive, Alexander says.
His job has been COVID-19 “100% seven days a week.”
“I got to point where I could no longer control communication through my email inbox, so I put a message on there, ‘I’m responding to the COVID-19 pandemic, so it may take me several days to get back to your email if it’s not related.’”
His coworkers were in the same situation. “It required our full and undivided attention,” he says.
The incident command team met three times a day, seven days a week for the first two months.
Kenny-Lynch never doubted her preparation. “This is what my job is on a daily basis,” she says. “COVID is my job on steroids.”
That said, it could be overwhelming, particularly as things changed so fast.
“Once you put something out, to educate, something [from the CDC] will come along the next day and you say, ‘OK, I take that back.’”
“Three hospitals, three different counties, three very different experiences,” says Wright, who leads the Bridgton and Rumford hospitals.
Bridgton Hospital, in Cumberland County, had an early surge of testing, and ultimately 14 positive cases, then cooled off. In Rumford, there was one positive test.
Wright was concerned that people who should be seeking medical care weren’t. He was right. “After about a month we started getting some pretty sick patients,” he says. “That’s the biggest fear, right? You do all this planning, then nothing happens. It’s human nature to let down your guard.”
On April 15, a digester at the Androscoggin Mill in Jay exploded and Rumford Hospital, the closest to the mill, was jolted into action.
“We heard about the explosion within moments,” Wright says. The hospital deployed its emergency response and got the ER ready.
The explosion happened at lunchtime, and mill workers were socially distancing by eating in their cars. No one was injured.
“That was a reminder to us, oh by the way, there’s other things going on besides COVID,” Wright says.
While CMMC has never had more than 10 patients in the COVID unit at a time, Alexander says the system did exactly what it should have.
“That’s how public health is supposed to work,” he says. “If you try to get ahead of things so it doesn’t become a big threat, you end up, in the rearview mirror, with ‘Why did they make such a big deal of that?’ The reason is because we don’t want it to become a really big problem.”
He says CMH, as well as the state, has done an effective job. “The bottom line is, we had prepared around a worst-case scenario and we were very fortunate that we never approached it,” he says.
CMH is now ready for whatever comes its way.
“We’re prepared to take on full capacity, that’s how we designed our process,” Alexander says. “We’re doing that because there has to be a recognition that the infection is still present in our community, we know that with certainty.”
Kenny-Lynch, who in January watched the blue dots spread across a graph while everyone else was going about their normal lives, agrees.
“As an epidemiologist, I feel like I can control what happens within these four walls,” she says. “What really frightens me, as a member of the community, are things outside of the hospital that I don’t have control of.”













0 Comments